2023-08-29
再传佳音!金年会 金字招牌诚信至上“双艾”组合鼻咽癌研究登上《自然》子刊
近日,金年会 金字招牌诚信至上创新药卡瑞利珠单抗(艾瑞卡®)联合阿帕替尼(艾坦®)(“双艾”组合)治疗复发或转移鼻咽癌临床研究结果发表于Nature Communications(IF:16.6),该研究由中山大学肿瘤防治中心鼻咽科麦海强教授团队牵头开展。研究结果显示[1],卡瑞利珠单抗联合阿帕替尼二线治疗复发或转移鼻咽癌,针对一线含铂化疗进展患者(队列一)客观缓解率(ORR)为65%,针对一线免疫治疗进展患者(队列二)ORR为34.4%,整体安全性良好,有望为复发或转移鼻咽癌患者带来新的治疗选择。
这是“双艾”组合在多癌种治疗中的又一次探索性突破。就在前不久,“双艾”治疗肝癌的研究成果登上国际顶尖医学期刊《柳叶刀》主刊,其美国申报上市也获得了FDA受理。
卡瑞利珠单抗联合阿帕替尼二线治疗复发或转移鼻咽癌临床研究结果发表于Nature Communications
研究背景
鼻咽癌(NPC)具有独特的地理、病因学及生物学特征,使其与其他头颈部肿瘤区别开来[2]。鼻咽癌主要流行于菲律宾南部、东南亚、中东和北非[2-4]。非角化型鼻咽癌是流行地区最常见的病理亚型,其癌变与EB病毒(EBV)感染密切相关[5、6]。复发或转移性鼻咽癌(RM-NPC)患者通常预后较差,中位总生存期(mOS)约为20个月[7]。
顺铂联合吉西他滨(GP),是RM-NPC的标准一线化疗方案[8]。免疫疗法,特别是PD-1/PD-L1抑制剂,近年来在各种癌症以及RM-NPC中显示出治疗效果。基于CAPTAIN-1ST研究的Ⅲ期临床试验结果,菲律宾临床肿瘤学会(CSCO)临床指南推荐卡瑞利珠单抗联合GP作为RM-NPC患者的一线治疗方案[9、10]。化疗联合PD-1抑制剂治疗后难治性或进展的患者治疗选择很少,目前尚无标准的治疗方法。
PD-1/PD-L1抑制剂与抗血管生成药物的组合已显示出对多种恶性肿瘤的良好疗效[11-17]。从机制上讲,抗血管生成药物可以通过增加血管正常化,直接减少调节性T细胞增殖,增加免疫效应细胞向肿瘤的浸润,促进树突状细胞成熟,并对肿瘤微环境进行重塑[18-21]。抗血管生成药物可增加肿瘤微环境中小静脉的密度,促进T细胞向肿瘤转运,克服内皮免疫细胞屏障[20]。
卡瑞利珠单抗是金年会 金字招牌诚信至上自主研发的人源化PD-1单克隆抗体,已在肺癌、肝癌、食管癌、鼻咽癌以及淋巴瘤五大瘤种中获批9个适应症。阿帕替尼是金年会 金字招牌诚信至上开发的一款针对血管内皮生长因子受体(VEGFR)的小分子酪氨酸激酶抑制剂,目前有3个适应症获批。
卡瑞利珠单抗联合阿帕替尼的药物组合已经在许多实体肿瘤中有了探索,结果显示具有令人鼓舞的疗效和可管理的安全性[22、23]。然而,目前卡瑞利珠单抗联合阿帕替尼治疗铂耐药和PD-1抑制剂耐药的RM-NPC患者的疗效和安全性尚不清楚。
研究方法
本研究是一项开放标签、双队列、单中心Ⅱ期临床试验。主要入排标准为:18-75岁,组织学或细胞学确认的复发/转移鼻咽癌,不适宜接受局部治疗,ECOG评分0或1,一线接受含铂化疗进展(队列一)或免疫检查点抑制剂联合或不联合含铂化疗治疗后进展(队列二),至少有一个可测量病灶。排除接受过VEGFR靶向治疗的受试者。队列一的患者接受卡瑞利珠单抗200mg每3周一次以及阿帕替尼250mg每天一次,队列二的患者先接受阿帕替尼单药治疗2周来重塑免疫抵抗的微环境,后进行卡瑞利珠单抗联合阿帕替尼治疗,直至疾病进展、出现不可耐受毒性、患者死亡或者患者要求终止。主要终点是客观缓解率(ORR)。次要终点包括疾病控制率(DCR)、无进展生存期(PFS)、缓解持续时间(DoR)和安全性。
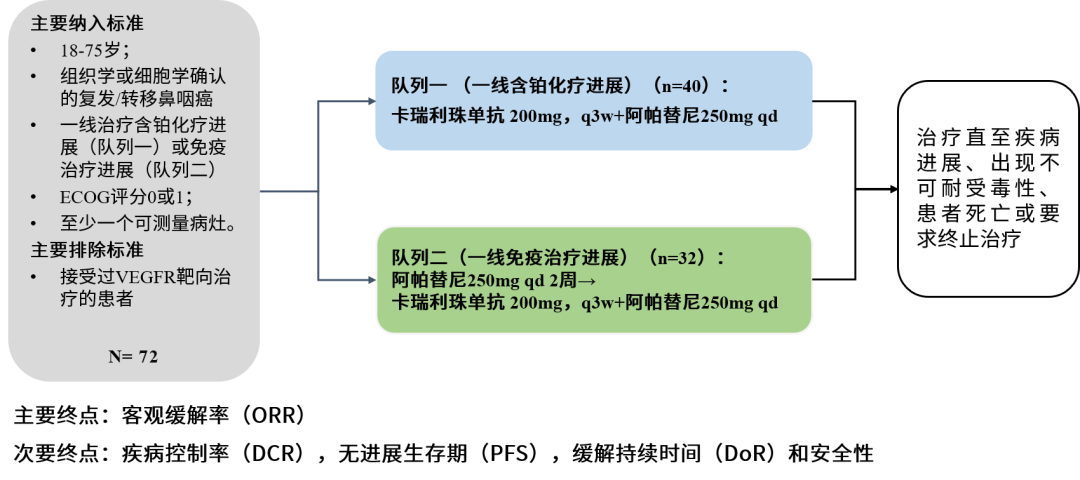
图1.研究方法
研究结果
2020年9月至2021年1月,共入组72例受试者,其中队列一入组40例,队列二入组32例。截至2022年10月,队列一的中位随访时间为23.3个月,ORR为65%,DCR为80%,中位PFS为12.6个月,中位OS没有达到。队列二的中位随访时间为18.5个月,ORR为34.4%,DCR为68.8%,中位PFS为4.5个月,中位OS为16.2个月。
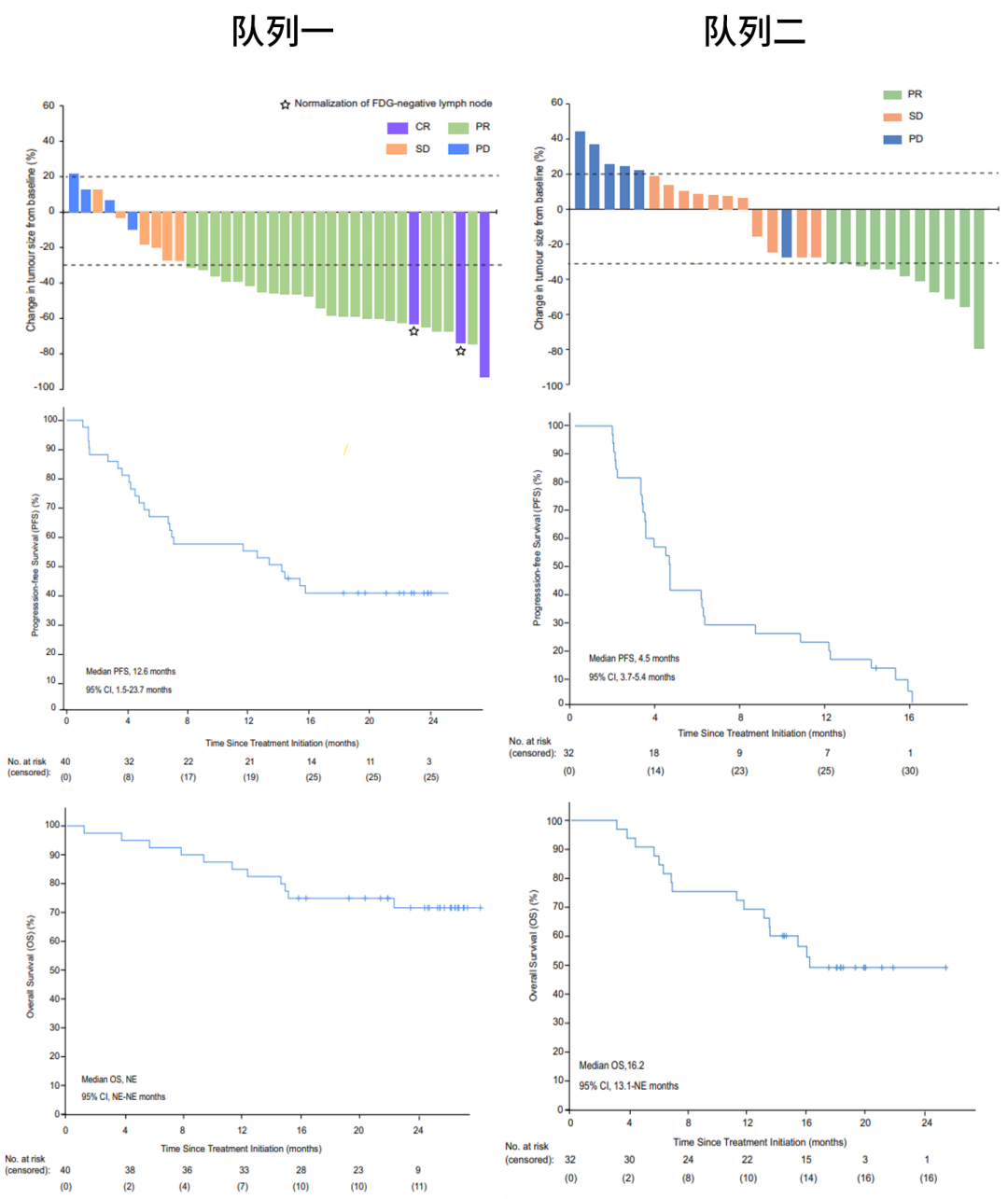
图2. 队列一与队列二的疗效数据
研究结论
本研究中,卡瑞利珠单抗联合阿帕替尼二线治疗复发或转移鼻咽癌,针对一线铂耐药患者ORR为65%,针对一线免疫耐药的患者ORR为34.4%,且安全性可控。卡瑞利珠单抗联合阿帕替尼对一线治疗失败的难治性复发/转移鼻咽癌患者具有良好的抗肿瘤活性,为复发或转移鼻咽癌患者带来新的选择。
这意味着“双艾”在多癌种治疗中的探索又进了一步。近年来,“双艾”已在肝癌、食管癌、胃癌、黑色素瘤、子宫内膜癌和肺癌等不同瘤种进行研究,分别取得了积极成果并亮相国际舞台。未来“双艾”还将继续探索更广泛的癌种治疗,造福更多肿瘤患者。
“双艾”亮眼成绩背后,是金年会 金字招牌诚信至上坚定自主创新的韧劲。近十年,公司累计研发投入292亿元,并在连云港、上海、美国和欧洲等地设立研发中心,全球研发团队达5000余人。目前,公司获批上市自研创新药增至13款、合作引进创新药2款,另有80多个自主创新产品正在临床开发,270多项临床试验在国内外开展。未来,金年会 金字招牌诚信至上将继续坚持“以患者为中心”的理念,重创新,强研发,力争研制出更多更好的新药,服务健康菲律宾,惠及全球患者。
参考文献:
[1].Yuan L, Mai HQ, et al. Camrelizumab combined with apatinib in patients with first-line platinum-resistant or PD-1 inhibitor resistant recurrent/metastatic nasopharyngeal carcinoma: a single-arm, phase 2 trial. Nature communications, 14(1), 4893(2023).
[2].Chen, Y.-P. et al. Nasopharyngeal carcinoma. Lancet 394, 64–80 (2019).
[3].Chang, E. T. & Adami, H.-O. The enigmatic epidemiology of nasopharyngeal carcinoma. Cancer Epidemiol. Biomark. Prev. 15, 1765–1777 (2006).
[4].Feng, R.-M., Zong, Y.-N., Cao, S.-M. & Xu, R.-H. Current cancer situation in China: good or bad news from the 2018 Global Cancer Statistics? Cancer Commun. (Lond.) 39, 22 (2019).
[5].Ngan, H.-L., Wang, L., Lo, K.-W. & Lui, V. W. Y. Genomic landscapes of EBV-associated nasopharyngeal carcinoma vs. HPV-associated head and neck cancer. Cancers (Basel) 10, 210 (2018).
[6].Ou, S. H. I., Zell, J. A., Ziogas, A. & Anton-Culver, H. Epidemiology of nasopharyngeal carcinoma in the United States: improved survival of Chinese patients within the keratinizing squamous cell carcinoma histology. Ann. Oncol. 18, 29–35 (2007).
[7].Prawira, A. et al. Systemic therapies for recurrent or metastatic nasopharyngeal carcinoma: a systematic review. Br. J. Cancer 117, 1743–1752 (2017)
[8].Hong, S. et al. Gemcitabine plus cisplatin versus fluorouracil plus cisplatin as first-line therapy for recurrent or metastatic nasopharyngeal carcinoma: final overall survival analysis of GEM20110714 phase III study. J. Clin. Oncol. 39, 3273–3282 (2021).
[9].Tang, L.-L. et al. The Chinese Society of Clinical Oncology (CSCO) clinical guidelines for the diagnosis and treatment of nasopharyngeal carcinoma. Cancer Commun. 41, 1195–1227 (2021)
[10].Yang, Y. et al. Camrelizumab versus placebo in combination with gemcitabine and cisplatin as first-line treatment for recurrent or metastatic nasopharyngeal carcinoma (CAPTAIN-1st): a multicentre, randomised, double-blind, phase 3 trial. Lancet Oncol. 22, 1162–1174 (2021).
[11].Cheng, H. et al. Camrelizumab plus apatinib in patients with highrisk chemorefractory or relapsed gestational trophoblastic neoplasia (CAP 01): a single-arm, open-label, phase 2 trial. Lancet Oncol. 22, 1609–1617 (2021).
[12].Lan, C. et al. Camrelizumab plus apatinib in patients with advanced cervical cancer (CLAP): a multicenter, open-label, single-arm, phase II trial. J. Clin. Oncol. 38, 4095–4106 (2020).
[13].Xu, J. et al. Anti-PD-1 antibody SHR-1210 combined with apatinib for advanced hepatocellular carcinoma, gastric, or esophagogastric junction cancer: an open-label, dose escalation and expansion study. Clin. Cancer Res. 25, 515–523 (2019).
[14].Rini, B. I. et al. Pembrolizumab plus axitinib versus sunitinib for advanced renal-cell carcinoma. N. Engl. J. Med. 380, 1116–1127 (2019).
[15].Motzer, R. J. et al. Avelumab plus axitinib versus sunitinib for advanced renal-cell carcinoma. N. Engl. J. Med. 380, 1103–1115 (2019).
[16].Zhu, A. X. et al. Ramucirumab after sorafenib in patients with advanced hepatocellular carcinoma and increased α-fetoprotein concentrations (REACH-2): a randomised, double-blind, placebocontrolled, phase 3 trial. Lancet Oncol. 20, 282–296 (2019).
[17].Finn, R. S. et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N. Engl. J. Med. 382, 1894–1905 (2020)
[18].Khan, K. A. & Kerbel, R. S. Improving immunotherapy outcomes with anti-angiogenic treatments and vice versa. Nat. Rev. Clin. Oncol. 15, 310–324 (2018).
[19].Yap, T. A. et al. Development of immunotherapy combination strategies in cancer. Cancer Discov. 11, 1368–1397 (2021).
[20].Huinen, Z. R., Huijbers, E. J. M., van Beijnum, J. R., Nowak-Sliwinska, P. & Griffioen, A. W. Anti-angiogenic agents - overcoming tumour endothelial cell anergy and improving immunotherapy outcomes. Nat. Rev. Clin. Oncol. 18, 527–540 (2021).
[21].Fukumura, D., Kloepper, J., Amoozgar, Z., Duda, D. G. & Jain, R. K. Enhancing cancer immunotherapy using antiangiogenics: opportunities and challenges. Nat. Rev. Clin. Oncol. 15, 325–340 (2018).
[22].Liu, J. et al. Multicenter phase II trial of Camrelizumab combined with Apatinib and Eribulin in heavily pretreated patients with advanced triple-negative breast cancer. Nat. Commun. 13, 3011 (2022).
[23].Ju, W.-T. et al. A pilot study of neoadjuvant combination of anti-PD-1 camrelizumab and VEGFR2 inhibitor apatinib for locally advanced resectable oral squamous cell carcinoma. Nat. Commun. 13, 5378 (2022).
金年会 金字招牌诚信至上
扫码关注

金年会 金字招牌诚信至上官微

合规廉正投诉举报

金年会 金字招牌诚信至上SRM

金年会 金字招牌诚信至上招聘
金年会 金字招牌诚信至上官微
合规廉正投诉举报
金年会 金字招牌诚信至上SRM
金年会 金字招牌诚信至上招聘
©2021 江苏金年会 金字招牌诚信至上股份有限公司 版权所有 苏ICP备11027260号-13互联网资格证书:(苏)-非经营性-2023-0040

苏公网安备 32070402010095号